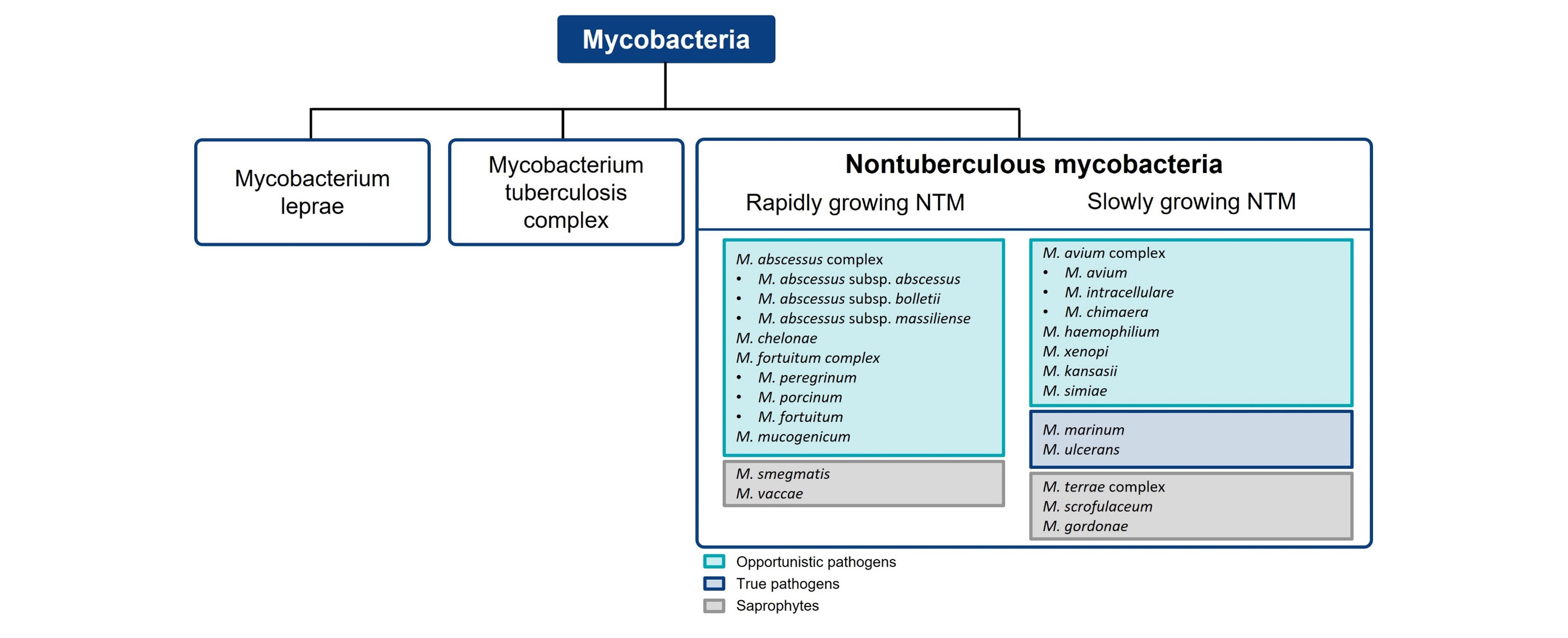
Microbiology
- Nontuberculous mycobacteria (NTM) species can be classified into slow and rapid growth subgroups1
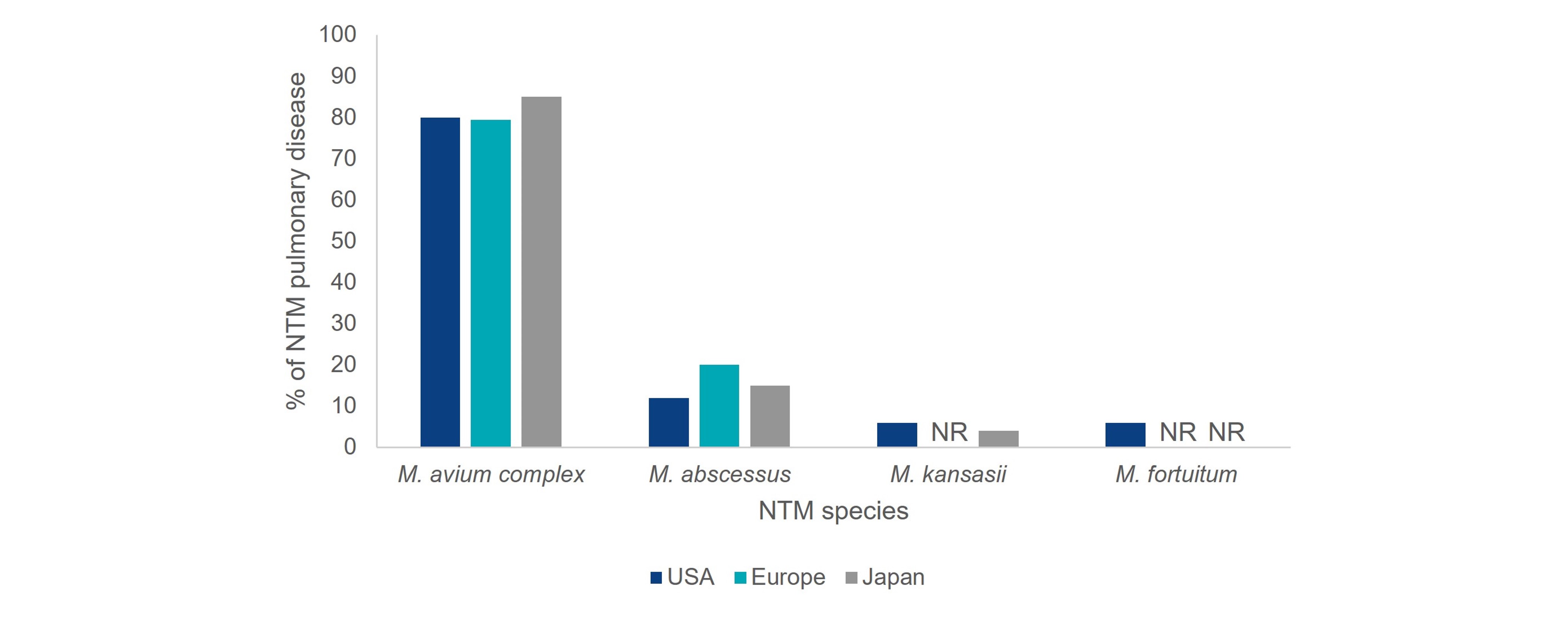
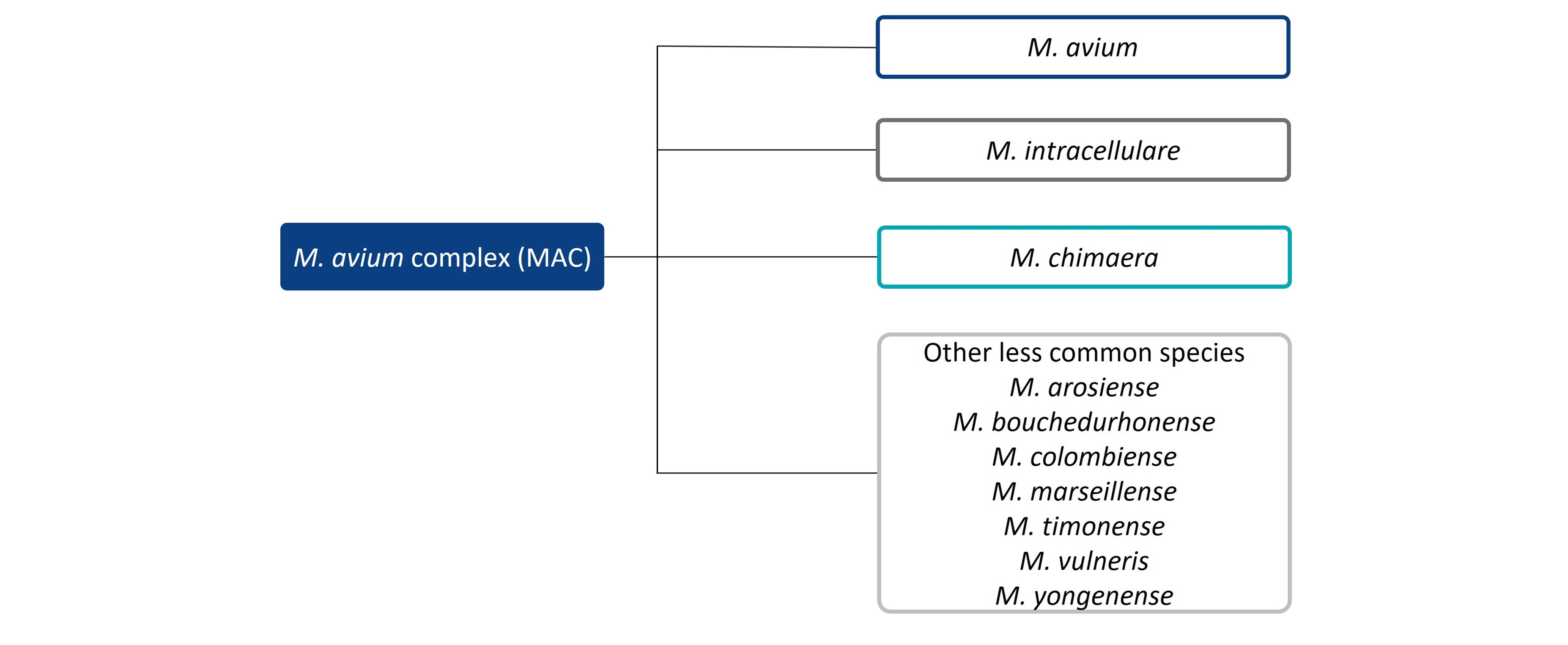
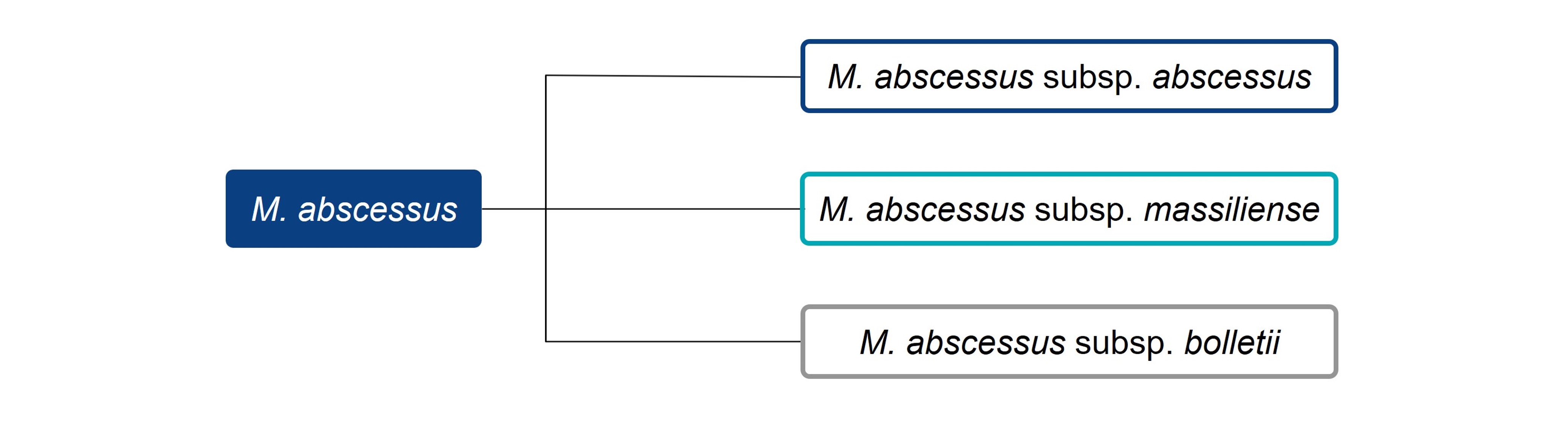
- Mycobacterium avium (M. avium) complex and Mycobacterium abscessus (M. abscessus) are the most common species causing pulmonary disease in these groups2,3
- The distribution of NTM species causing pulmonary disease varies by geographic region1,3
Image