Symptoms and Diagnosis
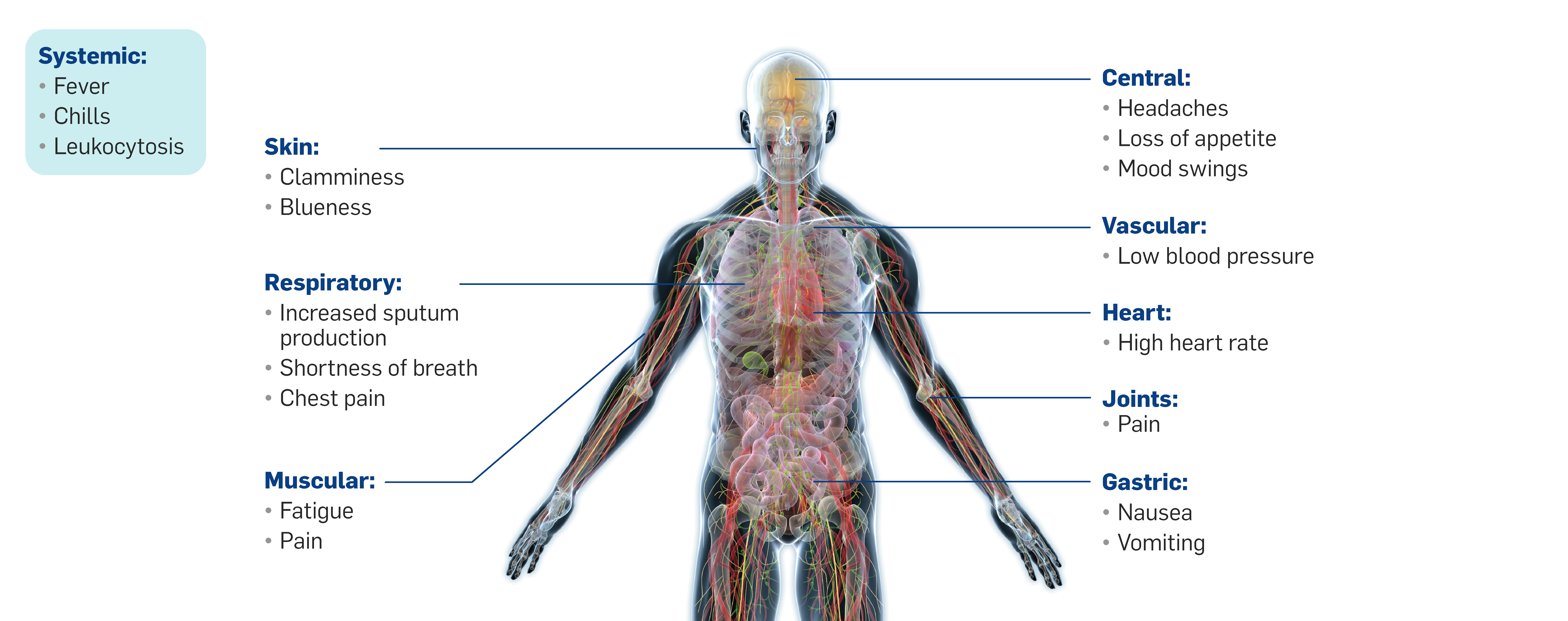
- Community-acquired pneumonia (CAP) presentation varies from mild pneumonia characterized by fever and productive cough to severe pneumonia characterized by respiratory distress and sepsis.1
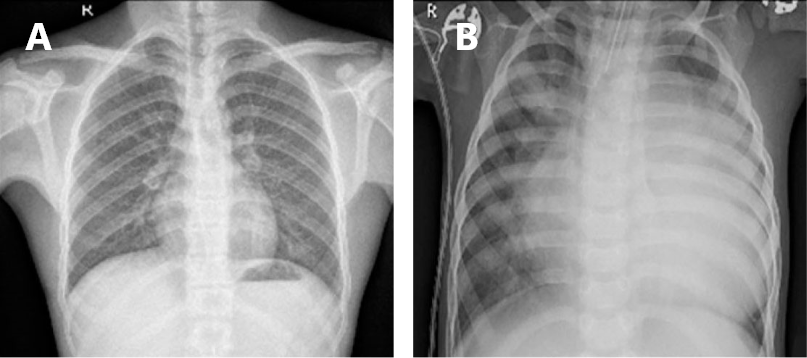
- Diagnosis of pneumonia includes assessment of clinical features and a demonstrable infiltrate by chest radiograph or other imaging technique.2
- Even with extensive microbiological testing a causative pathogen is never identified in most patients with CAP.3
Image