The spread of MRSA in the last decades has impacted the therapeutic approach for SSTIs which is reflected in the 2014 IDSA SSTI guidelines.12 The IDSA has also published guidelines that specifically focus on the treatment of MRSA infections including SSTIs.18 Additionally, the CDC has issued guidance on the outpatient management of SSTIs in the era of community-acquired (CA)-MRSA.19 The antibiotic treatment recommendations are consistent across the three documents, while the IDSA MRSA guidelines and CDC SSTI recommendations provide additional information about individual antibiotics that may assist clinicians in selecting the optimal treatment based on a variety of patient and disease characteristics.18,19
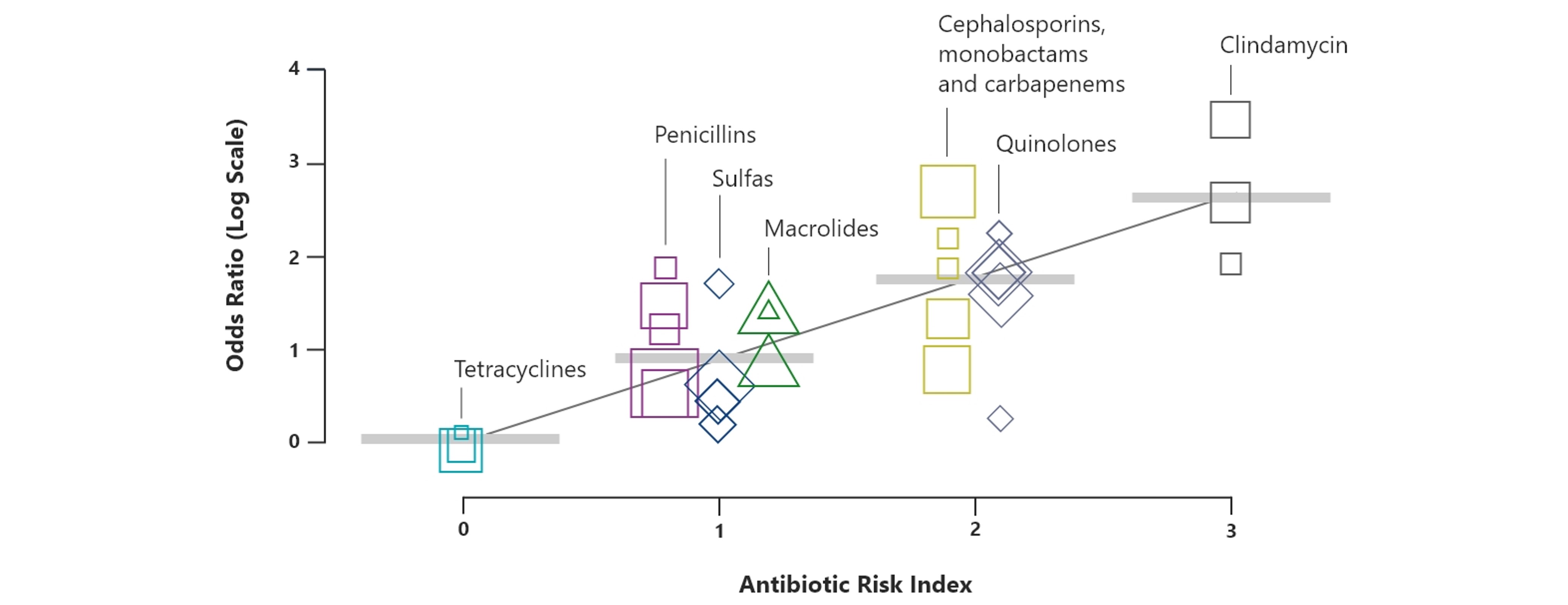
Adequate knowledge of the adverse effect profile of each antibiotic is important for guiding, monitoring, and managing adverse events to reduce the risk of toxicities that may negatively impact patient outcomes.2,3,12,20 Treatment may be complicated in patients with proven and serious allergies to beta-lactams and sulfonamides.21-23 Another potential challenge of antibiotic therapy is dose adjustments and drug monitoring. Many patients with SSTI have comorbidities and are older, which may affect drug pharmacokinetics and increases the risk for potential drug-drug interactions.24,25
Related to disease characteristics, the distinction between purulent and non-purulent SSTIs has a major impact on the recommended antibiotic treatment regimens with the IDSA SSTI treatment guidelines making a clear distinction between these two types of SSTI.12 However, in clinical practice this distinction is not always readily apparent to healthcare providers. Circumstances may prevent the culturing of purulent material when present or cultures may be obtained after an antibiotic was prescribed, leading to confusion about appropriate treatment.26
The IDSA SSTI guidelines also recommend an antibiotic that is effective against both MRSA and streptococci in patients whose cellulitis is associated with penetrating trauma, evidence of MRSA infection elsewhere, nasal colonization with MRSA, injection drug use, or severe infection.12 Therefore, clinicians often seek to prescribe an empiric treatment regimen with reliable activity against both streptococci and MRSA.27
The CDC recognizes the diagnostic uncertainty regarding MRSA and streptococci and provides additional guidance on the clinical management of MRSA in the community, with a focus on SSTIs.19